Report to/Rapport au :
Emergency and Protective Services Committee/
Comité des services de protection et d'urgence
16 May 2003 / le 16 May 2003
Submitted by/Soumis par: Steve
Kanellakos, General Manager/Directeur général Emergency and Protective
Services/Services de protection et d’urgence
Contact / Personne-ressource:
Anthony Di Monte,
Director, Emergency Medical Services / Directeur, Services médicaux d’urgence
580-2424 ext/poste 22458, Anthony.DiMonte@ottawa.ca
|
|
|
Ref N°:
ACS2003-EPS-EMS-0006 |
|
SUBJECT: |
Ottawa
Emergency Medical Services |
|
|
|
|
OBJET: |
SERVICES MÉDICAUX D’URGENCE D’OTTAWA |
REPORT
RECOMMENDATION
That the Emergency
and Protective Services Committee receive this report for information.
RECOMMANDATION
DU RAPPORT
Que le Comité des services de protection et
d’urgence prenne connaissance du présent rapport à titre d’information.
BACKGROUND
In 2000, Fitch &
Associates were contracted to develop the new Ottawa Emergency Medical Services
(EMS) system design. They proposed a
performance-based system focused on achieving a balance between quality and
cost with respect to customer satisfaction, clinical excellence, response time
reliability, economic efficiency, and public accountability through performance
reporting. This system design was
approved by the then, Regional Council in August 2000, and was implemented
January 1, 2001.
In developing a new system
design, Fitch & Associates focused on the enhancement of survivability
rates through the development of strategies to improve response times and to
increase capacity to treat patients on-scene.
Fitch & Associates determined that the previous system was comprised
of high quality and dedicated personnel but was characterized by severely
limited resources, primitive technology and a history of chronic under-funding.[1]
The new system design is a
performance-based system, or sometimes referred to as a high performance system
design, means that as an organization, Ottawa EMS is committed to measuring and
reporting on performance, and to being held to industry recognized performance
standards. It also reflects a
willingness to continuously evaluate and make improvements to all aspects of
the service.
A high performance system meets the needs of the users at the most economical cost to the taxpayers, and in such a way that can be measured against recognized industry standards. Achieving and maintaining a “high performance” system is viewed as our long-term, sustainable goal.
Operation Delta
Identified as a branch priority,
the Quality Assurance (QA) and Quality Improvement (QI) Set Up and
Implementation project commenced in 2001.
The mandate was to design, develop, and
implement a QA QI program for Ottawa EMS.
The goal of this QA QI program is to ensure that quality services are
delivered by every segment of the organization.
Concepts of Quality Assurance and Quality Improvement
Quality assurance and
quality improvement are often used interchangeably, but there is an important
distinction, particularly in a performance-based system. Quality Assurance refers to “all the planned or systemic actions
necessary to provide adequate confidence that a service or product will satisfy
given requirements for quality”[2]. Quality assurance activities are effective
in ensuring minimum standards are maintained.
Ottawa EMS can identify and correct deficiencies and shortcomings,
however these corrective actions are generally focused on maintaining the
established standards.
Quality improvement is “the process of attaining a new level of
performance and quality that is superior to any previous level of quality”[3]. Quality improvement is a more objective,
scientific method. It involves
developing performance indicators, establishing targets, collecting, organizing
and analyzing data, creating an action plan, evaluating the effectiveness of
the plan and communicating results.
The objective of quality
improvement is to strive for and achieve new
levels of success. Unlike quality
assurance, which measures against pre-determined standards, quality improvement
is about reaching new, previously unattained levels of performance. Quality improvement is a continuous process
of evaluating, adjusting and improving.
This process is often referred to as continuous
quality improvement (CQI).
Value of Performance Measures
Continuous Quality
Improvement (CQI) is focused on objectively measuring system performance for
the purpose of:
- Setting performance goals;
- Measuring performance to determine if desired performance targets
are met;
- Identifying gaps between current performance and desired
performance levels;
- Making adjustments to improve the system; and
- Measuring again.
Once performance targets are
met, Ottawa EMS may wish to elevate the minimum standards, by setting new
targets, or refocusing on other areas of performance within the system.
DISCUSSION
Quality Improvement Model
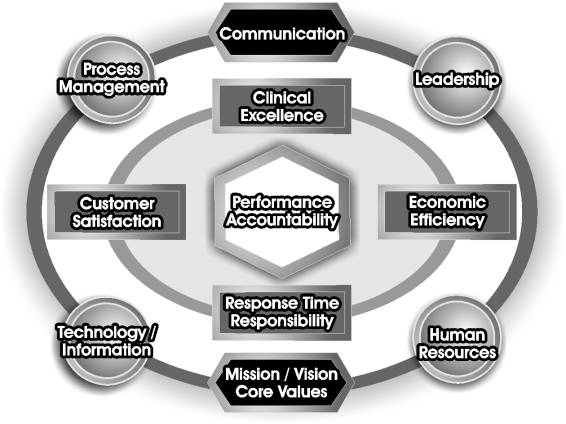
This model visual was
developed in the Fall of 2001 as a tool for increasing
understanding of the five key components of a performance-based system and
their relationship with a strategic vision, leadership and available resources.
Central to the model is performance accountability on all key components of the system. The other key components of a performance-based system are customer satisfaction, clinical excellence, economic efficiency, and response time reliability. Strong leadership, effective use of human resources and information technology, and design and utilization of efficient business processes will enable us to achieve our goals. And it is through a common vision and objectives, and a sound communication strategy that provides the framework for our organization.
Performance
Accountability
Prior
to amalgamation and the City of Ottawa’s assumption of land ambulance services in
January 2001, the Ministry of Health and Long Term Care (the Ministry) was responsible
for operating land ambulance services across the province. The Ministry accomplished
this by either directly managing ambulance services or contracting services to
private operators. Generally it was a
“level of effort” system, meaning operators provided the best service they
could, given the resources available. There were no specific
performance targets that had to be met in order to continue to operate the
service. One
of the important differences between a “level of effort” system and a
performance-based system is performance accountability through public
reporting.
Quality versus Quantity
Performance indicators must
be observable, measurable and achievable.
They should also be comparable over time, and hopefully with other EMS
services. The availability of data, and
the cost and practicality of collecting it must be taken into consideration. Often performance measures are limited to
collecting data on quantity of service rather than quality of
service. For example, reporting on call
volume is an indication of how busy Ottawa EMS may be, however it does not
indicate the quality of service provided.
Legislative Compliance
Within the EMS system, there
are provincial standards that Ottawa EMS is accountable for maintaining and
reporting on, or providing evidence of, on a regular basis. While primarily the Ambulance Act and
Regulations govern the ambulance service, Ottawa EMS is also regulated by the
following provincial legislation, standards and policies and procedures:
- Coroners
Act of
Ontario
- Employment
Standards Act of Ontario
- Mental
Health Act
of Ontario
- Occupational
Health and Safety Act
- Workplace
Safety and Insurance Act of Ontario
- Radio Act of Canada
- Health
Care Consent Act of Ontario
- Highway
Traffic Act of Ontario
- Regulated
Health Professions Act of Ontario
- Substitute Decision Maker’s Act of Ontario
- Central
Ambulance Communication Centre (CACC) Policies and Procedures
- Ottawa Base Hospital Program Policies, Procedures
- MOHLTC BLS
and ALS Patient Care Standards
- Ambulance Service
Documentation Standards
- Ambulance Service Certification Standards
- Ambulance Service Communicable Disease
Standards
- Ambulance Service Patient Care and Transportation Standards
- Land Ambulance & Emergency Response Vehicle Standard
- Provincial Equipment Standards for Ontario Ambulance Services
Examples of regular
reporting obligations to the Ministry are:
·
Level and type of service provided
·
Paramedic qualifications and maintenance of competencies
·
Staffing levels (Paramedics and Communication Officers)
·
Documentation standards compliance
·
Continuing Medical Education
·
Incident & Complaint investigations
·
Vehicles & patient care equipment procurement
Certification Process
The mandatory certification
process of the Ministry ensures that as an ambulance operator, Ottawa EMS is
meeting these obligations. In May 2001,
after only 5 months in operation, Ottawa EMS achieved an outstanding 91% rating
on its service review. The next service
review is tentatively scheduled for early 2004. Currently there are three Ottawa EMS paramedics serving as
members of the Ministry service review team, and participating in service
reviews of other services. This offers
an opportunity to observe first-hand how other services run their business and
to adapt and adopt best practices to this service.
Customer
Satisfaction
The first level of accountability
is to customers – the residents of Ottawa.
Now that Ottawa EMS is municipally operated and jointly funded with the
Province, accountability is “closer to home” - family, friends and neighbours -
the taxpayers of this community who are now funding in part, ambulance service
through their municipal taxes. As a
City of Ottawa service - visible on EMS vehicles and uniforms - also comes a
greater sense of ownership, and hopefully, pride from residents who care about
the service they receive from Ottawa EMS.
The Ottawa EMS Customer Service phone line is busy
with inquiries, compliments and concerns from residents about the service
provided on a daily basis. Ottawa EMS
has made a commitment to investigate and respond to customers in a timely
fashion. A Customer Relations Tracking
System (CRTS) has been established to track customer contacts.
Ottawa EMS has an opportunity
through public performance reporting and public education programs to influence
public expectations / perceptions about our service. This will include ensuring that the community has realistic
expectations of the service; that our performance goals are consistent with
community expectations and vice versa.
The challenge is to
demonstrate quantitatively and qualitatively that the service is provided in a
consistent, predictable and reliable manner.
It is essential that this is the perception of customers, in order for
customer satisfaction to be achieved.
Customer satisfaction can be achieved in part by the ability to meet or
exceed quantifiable (i.e. objective, measurable) expectations. An example of this is our ability to
demonstrate compliance with all applicable legislation, regulations, standards,
and policies that govern emergency medical services in the province of Ontario.
The Quality Improvement
Team within Program Development has a mandate to ensure regulatory compliance
by continually monitoring changes in regulations and reviewing our service to
ensure that our performance continues to meet standards.
It is the responsibility of
the Quality Improvement Team to develop and implement processes within the
Branch to ensure full public accountability for the investigation of all
complaints regarding any aspect of the delivery of the ambulance service. As a public agency, we are subject to
scrutiny by all stakeholders. This
scrutiny applies not only to the patient care, response time reliability,
economic efficiency, customer satisfaction, but also to the manner in which we
address and review internal and external complaints and concerns. An internal complaint investigation process
has been designed and implemented for thorough and objective investigations of
customer complaints. Responses from the
Director are sent to the customer, again demonstrating the level of commitment
we have to the customer.
Professionalism
All EMS staff has had the
opportunity recently to participate in a customized Professionalism
Workshop. The primary goal was to raise
awareness of professional attitudes and behavior and to provide staff with an
opportunity to share their perspectives on what constitutes professional behaviour
in EMS. A working group with representatives
from all divisions and all levels of our organization will be developing a
Professional Code of Conduct for our service, based on the feedback from these
workshops.
Clinical Excellence
Ottawa EMS is committed to
working collaboratively with the Base Hospital to develop and implement the
clinical aspects of the quality improvement program. Ottawa EMS and the Base Hospital have a signed Letter of
Agreement (since May 2001) that outlines the mutual desire to avoid duplication
of effort and to maximize the effectiveness of training programs and quality
improvement programs with combined resources.
Ottawa EMS’s system design
includes a move towards a full Advanced Life Support (ALS) paramedic
service. At end state, Ottawa EMS will
be composed of 60% Advanced Care Paramedics (ACPs) and 40% Primary Care
Paramedics (PCPs) so that there will be one ACP in attendance for each life
threatening (Code 4) call.
The Public Access
Defibrillation (PAD) Program, the largest program of its kind in Canada, has
placed 313 PADs in the community and provided for the training of 4,300 members
of the community in the use of the life-saving devices.
Ottawa EMS provides ongoing mass CPR Training. In 2002, EMS provided 4 sessions resulting in the training of approximately 250 individuals. In 2003, the goal is to offer 50 sessions throughout the year, and train approximately 4,000 individuals.
A variety of strategies
are being used to monitor and provide feedback on paramedics’ clinical
performance including:
Prospective Reviews:
- Primary EMS education and training (Ottawa EMS is represented on La Cité and Algonquin College
Advisory Committees)
- Recruitment and selection process
- Verification of paramedic qualifications upon hire, and tracking
of ongoing certification status (i.e. expiry dates)
- Continuing Medical Education (CME) and certification
- New employee orientation / training programs
- Returning employee reorientation programs (GRASP)
- Preceptor programs (for PCP and ACP students)
- Shift rotations through high and low-density areas to facilitate
adequate call volume to use skills.
Concurrent Reviews:
- Direct field observation / clinical evaluations (conducted by
Paramedic Team Leaders, Clinical Training Officers, and Quality Review
Officers)
- Indirect field observation (i.e. monitoring radio communication)
- Observation upon hospital arrival
- Verbal reporting skills.
Retrospective Reviews:
- Informal post call debriefings
- Direct medical control (patch reports)
- Chart reviews for accuracy and completeness
- Ambulance calls evaluations (ACE’s) conducted by the Base Hospital
to determine compliance with Base Hospital policies, patient care
protocols and standing orders
- Focused audits
- Incident reports and investigative reviews
- Clinical skill inventory.
Patient
Care Database
Patient
care information is currently collected by various paper-based methods
including ambulance call reports, incident reports, Base Hospital patch
reports, Base Hospital ambulance call evaluations and electronic data from
defibrillators.
A comprehensive patient information management system
is being developed to enable reports based on tangible information to review
and monitor the performance and competencies of paramedics and patient
outcomes. We are critically evaluating
the current patient care data collection process to identify opportunities for
improving the process utilizing electronic data collection, an emerging best
practice in the EMS industry.
Data from ambulance call
reports (emergent calls) have been collected since January 2002. Ottawa EMS is
currently working with the City of Ottawa ITS to replace the current database
with an in-house developed database, which will be linked to ARIS (Ministry
dispatch data), and will be designed for more flexible reporting of:
- Successful performance of procedures (e.g. at system level and for
individual employee performance)
- Procedure statistics (at system level and for individual employee
performance)
- Patient outcome for primary problems
- Dispatch complaint codes / priority codes versus final problem /
return priority
- Ambulance call report completion and compliance (i.e. compliance
with Ministry standards).
Clinical performance
measures, the paramedic performance monitoring system and the patient care
database will drive the focus of training and development programs in order for
Ottawa EMS to meet it’s clinical performance objectives.
Patient Care Equipment
Advances in medical care are
bringing about rapid changes in technology and requirements for
state-of-the-art equipment. A part of
Ottawa EMS’s quality improvement program is establishing an Equipment Committee
responsible for developing an equipment review process for current and new
equipment. This committee is
responsible for evaluating and recommending medical equipment for use within
the EMS Branch. Another Medical
Equipment Committee is established as part of the Medical Services “Centre of
Expertise” role that EMS has assumed for the City of Ottawa. This committee is responsible for making
recommendations for the standardization of medical equipment across the
corporation.
Pre-hospital Research
Another
important aspect of our quality improvement program is participation in
research and staying current with medical research related to EMS – such as
drugs and treatment modalities that have the greatest influence on stabilizing
patients, shortening patient hospitalization, and reducing patient morbidity
and mortality.
Currently Ottawa EMS is participating in the following medical research
projects:
1.
Ontario Pre-hospital Advanced Life Support (OPALS)
study
2.
The Canadian C-spine Rule Pre-Hospital Study
3.
Capital Acute Myocardial Infarction (AMI)
Study
4. Canadian Stroke Network (Director EMS is a board member).
Findings that arise from these and other studies will drive further
research to address and focus patient care and protocols within the EMS system.
Economic Efficiency
Achieving a
balance between quality service and cost, and ensuring high performance across
the system is an ongoing challenge facing all EMS systems.
Measuring performance allows Ottawa EMS the opportunity to compare its service with other comparable EMS systems (i.e. ensuring ‘apples to apples’ comparisons). Ottawa EMS is currently participating in the Ontario Municipal Benchmarking Initiative (OMBI) and the National Benchmarking Initiative (under the auspices of the Canadian EMS Directors and Chiefs Association) to identify and develop appropriate service specific performance measures, capture performance data, and analyze and benchmark results, in order to identify best practices of service efficiency and quality in EMS. Some of the benchmarks currently being tested include:
- Gross cost per vehicle hour (efficiency measure)
- Vehicle Unit Hour Utilization (productivity measure)
- 90th percentile response time to life threatening calls
(effectiveness measure)
·
% ALS call response (effectiveness measure)
EMS Headquarters
The EMS Headquarters is
conceivably the most significant change from the “level of effort” system to
the “performance-based” system. This
headquarters allows for efficient and effective use of supervisory staff,
vehicle and equipment maintenance (stocking & cleaning) and the
centralizing of logistics support staff.
This system design was determined to be the most economical way to
provide service to the City of Ottawa, and is now recognized as a best practice
nationally.
Preventative Maintenance
Economic efficiency as it relates to the maintenance of vehicles and
equipment within Ottawa EMS is achieved through the preventative maintenance
program. Preventative maintenance
ensures that all Ottawa EMS equipment is maintained in a timely manner and to
the intervals recommended by the Manufacturer.
Ottawa EMS has assumed responsibility for the preventative maintenance of
all patient care equipment and accessories (e.g. stretchers, stair chairs,
oxygen equipment). A new biomedical
engineer technologist position will provide preventative
maintenance, inspection, servicing, quality assurance, and records management
for all EMS biomedical equipment.
Response
Time Performance and Reliability
Under the Land Ambulance Certification Standards,
Ottawa EMS must –
(b.1) Establish and maintain a 90th percentile Response Time Performance
Standard for the applicant's land ambulance service for priority four emergency
calls, and
(b.2) Where
a response time standard is set under clause (b.1), that standard will be
reported to the Director, Emergency Health Services Branch not less than 30
days prior to commencing the provision of service and subsequently, not less
than 30 days prior to the beginning of each calendar year, and
(b.3) The response time standard set under clause
(b.1) and reported under clause (b.2) shall not be of a longer time duration
than the 90th percentile response
time standard for priority four emergency calls set by the operator who
provided land ambulance and emergency response service in the area in 1996.
[4]
A continuous need to meet all
legislative requirements set out by the Ministry, the Ambulance
Act and other legislation is
an ongoing commitment to Ottawa Emergency Medical Services. This is directly related to the City
maintaining its authority to operate an EMS service.
Ottawa EMS, through Ottawa Council, has made a commitment to the citizens of Ottawa to establish (over a three year period) and maintain a 90th percentile response time for priority four calls of 8:59 minutes.
|
Dispatch
Priority |
Zone |
1996 |
By
end of 2001 |
By
end of 2002 |
By
end of 2003 |
|
Code 4 |
-High
Density -Low Density |
14:28 22:30 |
12:59 18:59 |
10:59 16:59 |
8:59 15:59 |
Total calls responded to by
EMS has increased by 10% from 2001 to 2002, with a 17% increase in Code 4 (life
threatening) calls:
|
|
2001 |
2002 |
|
Code 4 (Life Threatening) |
36,753 |
42,915 |
|
Code 3 (Urgent) |
20,662 |
22,601 |
|
Code 2 (Scheduled) |
4,578 |
4,873 |
|
Code 1 (Non urgent) |
10,457 |
9,467 |
|
Total requests for service |
72,450 |
79,856 |
During this same period of
time Ottawa EMS achieved a response time of 10:50 (90% of the time) in the High
Density area and 16:30 (90% of the time) in the Low Density areas.
Ottawa EMS is continually striving to reduce
response times at the same time as facing increased demand on services related
to a growing and ageing population. Ottawa's population is
projected to grow by up to 50 per cent by 2021[5].
And during this same time frame, it is estimated
that the proportion of the population aged 65 and over will be at an
unprecedented 15 percent.[6]
Factors that have contributed to improved
response time reliability and enhanced patient care include:
·
Increasing
the number of emergency response units from 39 to 52
·
Increasing
our staffing availability by increasing the number of paramedics from
221 to 261
·
An increase
in unit hour availability from 195,000 to 206,000 hours
·
Continuous
refinements to the deployment plan
·
Strategic
use of EMS resources such as specialty teams
·
Assumption
of dispatch (a key component of the fundamental system design).
A flexible deployment plan was
implemented in September 2002. The
deployment plan prioritizes post locations to provide those areas with the
greatest historical call demand the highest priority, in order that resources
are available when and where they are needed. Scheduling of paramedics is based
on call volume to match demand patterns.
A conversion to a full time staffing
model and the implementation of a corporate initiative to manage sick leave,
all in an effort to increase availability of paramedics to staff vehicles have
been established.
Technology and Information
Technology is a tool to be used
to support our business processes for greater efficiency. Decision-making should be based on reliable,
sound data, and not on intuition or individual perspectives. Historically, ambulance operators have
relied on the Base Hospital for this data management, particularly with regards
to clinical aspects of the service. The
EMS quality improvement program will ensure that we are collecting, managing
and reporting on our own performance data.
Data collection and reporting
systems (information technology) are currently being utilized and will continue
to be expanded for key performance indicators to support decision-making and
strategic planning, and to facilitate comparisons of performance with other EMS
services. Current databases include:
·
Emergency Medical Equipment Tracking (EMET)
·
Vehicle Assignment and Tracking (VAT)
·
Ambulance Response Information System (ARIS)
dispatch database
·
Patient care database
·
People Soft (Human Resources database)
·
Client Request Tracking System (CRTS)
·
Automated Vehicle Location (AVL)
·
Telestaff
(Automatic scheduling- shift-scheduling efficiency).
Process Management
An outcome of another EPS Operation Delta Project: Design / Enhance
Business Processes was the identification and evaluation of key processes that
support EMS operations to ensure that the critical functions were designed and
refined to meet the needs of internal / external customers. Thirty-six core business processes have been
identified and plotted on flowcharts, and key linkages between processes
developed.
As
part of the process engineering, process quality measures continue to be
identified (key indicators) based on internal and external customer
requirements and established standards and control strategies to keep processes
within standards.
CONCLUSION
The Ottawa EMS system is a
complex system. As this performance-based
system evolves, performance indicators will need to re-evaluated in relation to
the changing legislative, demographic, and fiscal environment which creates
pressures that require increase in resource levels to maintain service
commitments. The ability of the system
to capture and utilize these outcomes will provide a powerful tool for the
future direction of the system.
Ottawa EMS is committed to
progressive and proactive quality improvement programs and initiatives, that will
simultaneously deliver clinical excellence, response time reliability, economic
efficiency, customer satisfaction, and performance accountability undertaking
to measure and report its performance, while being held to industry recognized
performance standards.
CONSULTATION
All
Ottawa EMS Divisions were consulted for this report
FINANCIAL IMPLICATIONS
There are no financial
implications associated with this report.